

Background: Secondary CNS B-cell lymphomas (SCNSL) are aggressive lymphomas with a very poor prognosis. Genetic subtypes of DLBCL with CNS tropism are enriched for chronic active B-cell receptor signaling and may respond to BTK inhibition (BTKi). CLL, MCL, and transformed lymphomas can also involve the CNS and are BTKi responsive. TEDDI-R achieves durable remissions in relapsed/refractory primary DLBCL of the CNS (PCNSL) but the profile of SCNSL tumors that are ibrutinib-responsive is unknown. We present preliminary results from a response-adapted trial of ibrutinib with TEDD-R in SCNSL.
Methods: Pts with aggressive B-cell lymphomas with secondary CNS involvement are eligible if age ≥18 and adequate organ function. Pts must have relapsed after frontline therapy or can be untreated if brain parenchyma involved. Prior BTKi is allowed, but HIVinfection and EBV+ lymphomas are excluded. Baseline tests include brain MRI, FDG-PET brain and body, CSF with flow cytometry, Ommaya, and eye exam. Pts receive isavuconazole starting at 200mg BID x 3d prior to ibrutinib to prevent fungal infections associated with TEDDI-R and then 200mg daily unless ibrutinib stopped. Pts first receive ibrutinib 560mg daily x 14d in a window. If ≥20% reduction after ibrutinib, pts receive TEDDI-R for 4 cycles every 21d with IT cytarabine. Pts with <20% reduction after ibrutinib receive TEDD-R without ibrutinib for 4 cycles every 21d with IT cytarabine. No consolidation or maintenance is permitted. Surveillance for fungal infections includes chest CT after each cycle along with Beta-D glucan and aspergillus galactomannan in blood and CSF. Brain MRI and CT scans are performed after cycles 1, 2, and 4 to determine response. All remissions by MRI are confirmed with FDG-PET and CSF analysis. Surveillance brain MRI and CT scans are q3m for 1y, q4m x 1y, q6m x 1y, then annually.
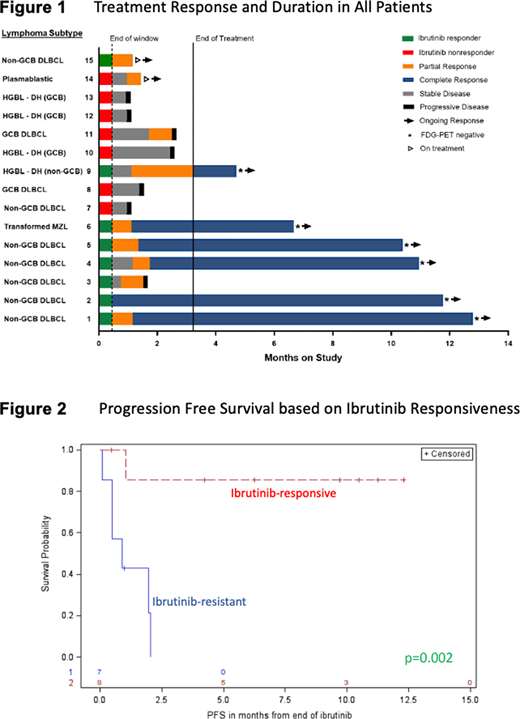
Results: 16 pts with a median age 67 (range 40-79) enrolled between June 2019 and July 2020. 15 (94%) pts had DLBCL comprising 9 (60%) non-GCB, 5 (33%) GCB, and 1 (7%) transformed from MZL. One pt had plasmablastic lymphoma. Eight (50%) pts had a MYC-rearrangement including 4 (25%) with both MYC and BCL2 or BCL6 rearrangements. Eight (50%) pts had isolated CNS disease and 8 (50%) had synchronous CNS and peripheral disease. All pts relapsed after a median of 2 (range 1-4) prior therapies and all (100%) pts received prior anthracycline. Seven pts (44%) had prior CNS prophylaxis and 8 pts (50%) had prior HD-MTX based salvage therapy. Toxicity was evaluated across 35 cycles. G3 and G4 neutropenia occurred in 49% and 29% of cycles, respectively, while febrile neutropenia occurred in 9% of cycles. The median (range) duration of neutropenia was 6 (1-13) days. Five (14%) cycles were complicated by ≥G3 infection, but no opportunistic infections (including Aspergillus) were observed. One pt developed a bacterial infection during cycle 1 and died. G3 and G4 thrombocytopenia occurred in 34% and 23% of cycles, respectively, and 1 pt developed G3 hematuria. G3 mucositis occurred in 9% of cycles and palmar-plantar-erythrodysesthesia led to dose reductions of liposomal doxorubicin in 5 (36%) pts. Of 15 pts who completed the 14d ibrutinib window and were evaluable, 8 (53%) were ibrutinib-responsive and 7 (47%) were ibrutinib-resistant (Figure 1). Clinical responses were concordant across anatomic compartments; of 8 pts with both CNS and peripheral disease, 5 (63%) responded to ibrutinib in both compartments while 3 (37%) did not respond in either compartment. All 8 ibrutinib responders had a non-GCB phenotype and six (75%) achieved CR. One died of treatment-related toxicity after a PR and 1 is still on therapy. Only two (29%) pts with ibrutinib-resistant tumors achieved PR and none have achieved CR. After a median follow-up of 5.1m, a landmark analysis starting after the ibrutinib window demonstrated the PFS for pts with ibrutinib-responsive compared to ibrutinib-resistant tumors was not reached vs. 0.9m (95% CI: 0.1-2m)(p=0.002)(Figure 2).
Conclusions: Patients with SCNSL tumors that are ibrutinib-responsive achieve a high rate of complete response to TEDDI-R in both CNS and peripheral disease. Patients with tumors that are ibrutinib-resistant also respond poorly to TEDD-R. Toxicity is mainly hematologic, and no Aspergillus infections have occurred with the use of isavuconazole prophylaxis. Updated clinical results from this ongoing study (NCT03964090) and will be presented at the meeting.
No relevant conflicts of interest to declare.
ibrutinib for use in secondary cns lymphoma as part of a clinical trial

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal